
The AI Question Nobody in Medicine Is Asking
This post may contain links from our sponsors. We provide you with accurate, reliable information. Learn more about how we make money and select our advertising partners.
Here's the thing that's been bugging a lot of physicians about the whole AI-in-medicine conversation.
Everyone keeps asking the same question: Will AI replace doctors?
It's the scary headline. Understandable. But there's a bigger, more uncomfortable question sitting right underneath it that almost nobody is talking about.
Who owns the AI layer, and will physicians have any say in it?
Disclaimer: While these are general suggestions, it's important to conduct thorough research and due diligence when selecting AI tools. We do not endorse or promote any specific AI tools mentioned here. This article is for educational and informational purposes only. It is not intended to provide legal, financial, or clinical advice. Always comply with HIPAA and institutional policies. For any decisions that impact patient care or finances, consult a qualified professional.
AI in medicine isn't a future thing anymore. It's already inside the hospital. It's reading imaging studies, flagging sepsis alerts, pre-populating clinical notes, pushing prior auth recommendations, and in some systems, determining how long a patient visit should take.
And in most cases, nobody asked the doctors.
The hospital system bought the platform. A tech company trained the model. A committee somewhere approved the rollout. The physicians showed up to clinic and it was just there.
That's not a coincidence. It's a pattern. And it's one worth paying close attention to.

The Real Power Shift Isn't About Jobs. It's About Control.
The replacement conversation mostly misses the point.
Are some tasks going to be automated? Absolutely. Radiology reads, pattern recognition, screening interpretations, documentation. A lot of that is already happening or close to it. But wholesale replacement of physicians isn't what most people working in this space actually expect, at least not in any near-term way.
What's more likely, and already underway, is something subtler. The AI doesn't replace the doctor. It just sits between the doctor and the decision.
Think about prior authorizations. AI systems are now making recommendations on whether treatments get approved before any physician conversation happens. Some hospital systems use AI-generated productivity scores to evaluate physician performance. Documentation tools summarize patient visits in ways that may or may not reflect what was actually said or meant.
The doctor is still on paper. But the system around them is getting smarter, faster, and more opinionated.
And who built that system? Who fed it the data? Who decided what it was optimizing for?
Not the physicians.
This isn't an argument that AI is bad. A lot of it is genuinely useful. But useful and neutral are two different things. Every AI system reflects the priorities of whoever built it and paid for it. In most hospital contexts, that's not the physician.
That's the shift. Not replacement. Repositioning.
Physicians Are Sitting Out the Conversation That Matters Most
Here's where it gets frustrating.
The doctors who are going to shape how AI gets used in medicine aren't necessarily the best clinicians. They're the ones who got in early, learned the tools, built relationships with the companies, and have a seat at the table.
Right now, a lot of that is happening without physicians in the room.
The AI companies building for healthcare aren't waiting for doctors to weigh in. They're moving fast. They're talking to hospital administrators, insurance companies, and private equity groups. They're pitching systems that reduce costs and increase throughput, which are valid goals, but they're not the same as goals that center physician judgment or patient outcomes.
Doctors haven't engaged more for understandable reasons. The workload is brutal. Years of training were spent learning to take care of patients, not sit on advisory boards for software companies. Most physicians aren't thinking about this stuff between a full patient load and getting home to their families.
But that absence has a cost.
The physicians engaging with AI, not just using it but actually understanding how it works, what it can't do, and where it gets things wrong, those are the ones who will have influence over how this plays out. Everyone else will find that the system already decided for them.
This pattern isn't new. It's the same one that played out with insurance companies, hospital systems, and private equity. Every time a new power entered medicine, the physicians who were financially independent, who had options, who weren't trapped by a single employer, were the ones who could push back, speak up, or build something else.
Financial independence doesn't just provide freedom from a bad job. It provides the ability to stay in a fight worth having.
Financial Independence Is Now Part of Your AI Strategy
That connection might sound like a stretch. It isn't.
A physician financially dependent on a single employer, one that's rolling out an AI system changing how performance is measured, how notes are reviewed, how productivity is benchmarked, has very limited options. Adapt to the system or risk the income.
That's not hypothetical. It's already happening in some hospital systems.
But a physician who's built passive income, real estate cash flow, or other income streams that don't require showing up anywhere, has a different kind of leverage. Not over the AI itself, but over their own choices. The ability to say no to a contract requiring a documentation system that doesn't feel right. The room to take a pay cut to join a smaller group that operates differently. The option to step back from clinical medicine on their own terms, not because of burnout or a forced exit.
The reason more physicians aren't asking harder questions about who controls the AI layer is at least partly because too many feel like they can't afford to.
That's the real connection. Financial independence isn't just about retiring early or buying back time, though it's both of those things too. It's about staying in a position to have a voice when the decisions that shape medicine are being made.
Right now, those decisions are being made fast.
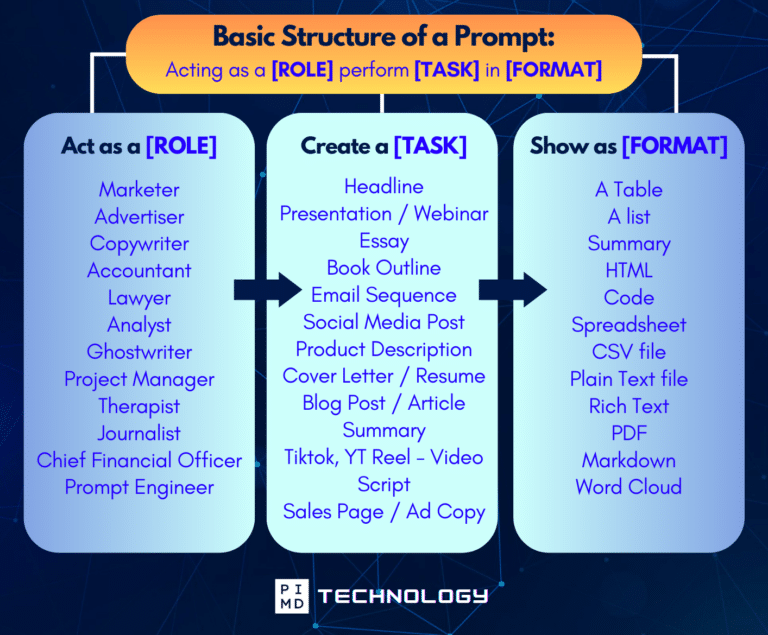
Unlock the Full Power of ChatGPT With This Copy-and-Paste Prompt Formula!
Download the Complete ChatGPT Cheat Sheet! Your go-to guide to writing better, faster prompts in seconds. Whether you're crafting emails, social posts, or presentations, just follow the formula to get results instantly.
Save time. Get clarity. Create smarter.
Final Thoughts
AI in medicine isn't going away, and it probably shouldn't. There's genuinely useful stuff here, and the physicians who engage with it seriously will be better positioned than the ones who don't.
But “AI is useful” and “AI will be used in your best interest” aren't the same sentence.
The physicians with the most say in how this plays out will be the ones who are informed, financially free enough to push back, and engaged early enough to matter. Everyone else will show up one day and find a lot of decisions have already been made.
It's happened before. The pattern is pretty recognizable by now.
So just curious… are you paying attention to how AI is being used in your hospital or practice? Have you had any say in it at all?
I'd genuinely love to hear what you're seeing out there. Comment below and let me know.
Download The Physician’s Starter Guide to AI – a free, easy-to-digest resource that walks you through smart ways to integrate tools like ChatGPT into your professional and personal life. Whether you're AI-curious or already experimenting, this guide will save you time, stress, and maybe even a little sanity.
Want more tips to sharpen your AI skills? Subscribe to our newsletter for exclusive insights and practical advice. You'll also get access to our free AI resource page, packed with AI tools and tutorials to help you have more in life outside of medicine. Let’s make life easier, one prompt at a time. Make it happen!
Disclaimer: The information provided here is based on available public data and may not be entirely accurate or up-to-date. It's recommended to contact the respective companies/individuals for detailed information on features, pricing, and availability. All screenshots are used under the principles of fair use for editorial, educational, or commentary purposes. All trademarks and copyrights belong to their respective owners.
If you want more content like this, make sure you subscribe to our newsletter to get updates on the latest trends for AI, tech, and so much more.
Further Reading
Disclaimer: The topic presented in this article is provided as general information and for educational purposes. It is not a substitute for professional advice. Accordingly, before taking action, consult with your team of professionals.

